
by Justin Jackson, Medical Xpress
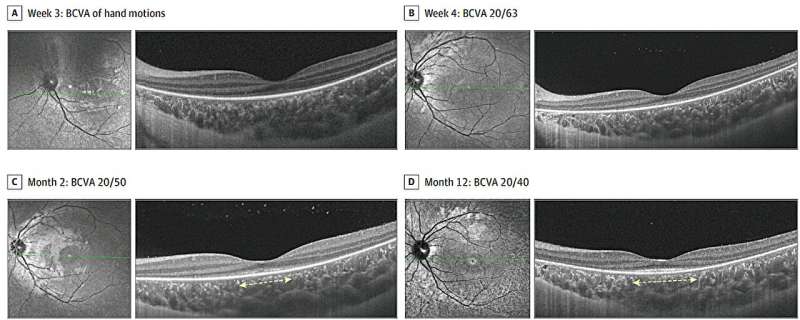
A 6-year-old girl presented with hyperacute vision loss after a fever, with a best-corrected visual acuity (BCVA) of hand motions in both eyes. The ellipsoid zone (EZ) and external limiting membrane (ELM) were blurred at week 3 (A) and gradually clarified at week 4 (B), were restored but disrupted at month 2 (C), and showed tapered foveal EZ with ELM (flying saucer sign) at month 12 (D). The dashed line indicates disrupted EZ; solid line, intact EZ. Credit: JAMA Ophthalmology (2025). DOI: 10.1001/jamaophthalmol.2024.6372
A multicenter study led by researchers from the State Key Laboratory of Ophthalmology in China has characterized a distinct retinal disorder in children following high fever illness. The study describes hyperacute outer retinal dysfunction (HORD), a condition marked by sudden bilateral vision loss, photoreceptor disruption, and variable recovery.
Eight pediatric patients between the ages of 3 and 7 experienced severe, sudden-onset vision loss approximately two weeks after a febrile illness. Despite initial poor visual acuity, most showed significant central vision recovery over one year. Comprehensive retinal imaging revealed characteristic ellipsoid zone (EZ) and external limiting membrane (ELM) disruptions. Electroretinography (ERG) findings demonstrated extinguished cone and rod responses, even in cases where vision improved.
In the study, "Hyperacute Outer Retinal Dysfunction, " published in JAMA Ophthalmology, researchers examined eight children (16 eyes) referred to pediatric retina services in China. Patients had no prior history of visual impairment and underwent thorough ophthalmic and systemic evaluations. Exclusion criteria included inherited retinal disease, uveitis, and white dot syndromes.
Best-corrected visual acuity (BCVA) was assessed at baseline and during follow-up. Multimodal imaging included color fundus photography, ultra-widefield imaging, optical coherence tomography (OCT), fluorescence angiography, fundus autofluorescence, and electroretinography. Genetic and serological testing was conducted to rule out inherited and autoimmune retinal diseases. Patients received varying immunosuppressive treatments, including corticosteroids, intravenous immunoglobulin and methotrexate.
Initial symptoms included severe bilateral vision loss, nyctalopia, visual field constriction, and dyschromatopsia. At presentation, the patient's mean visual acuity was below the ability to count fingers correctly. OCT imaging showed diffuse EZ and ELM loss, while early fundus findings were largely unremarkable.
By the fourth week, signs of macular recovery appeared. At one year, 88% (7 of 8 patients) achieved visual acuity of 20/40 or better, with 50% (4 of 8) reaching 20/25 or better. Macular EZ and ELM appeared intact in 75% and 88% of eyes, respectively, though extrafoveal regions remained affected. ERG continued to show extinguished rod and cone responses despite visual improvement.
Systemic evaluations were unremarkable. No infectious or autoimmune triggers were identified, although two patients tested positive for specific antiretinal antibodies (antiPKC γ and antiRi). Treatment with corticosteroids and IVIG was initiated in most patients, though a definitive therapeutic effect of treatment remained unclear from the study.
A commentary by Timothy Boyce and Ian Han at the University of Iowa, "Hyperacute Outer Retinal Dysfunction—A Retina on Fire, " also published in JAMA Ophthalmology, suggests that HORD may represent a novel inflammatory-mediated retinal disorder.
The authors propose similarities with autoimmune encephalitis, suggesting a possible antibody-mediated mechanism. Early OCT findings, including vitritis, vascular sheathing, and intraretinal hyperreflective dots, point to acute inflammation as a potential driver of retinal damage.
Comparison with existing retinal diseases highlights HORD's distinct features. Unlike multiple evanescent white dot syndrome (MEWDS) or acute zonal occult outer retinopathy (AZOOR), HORD presents with severe bilateral involvement and only partial recovery. While some characteristics overlap with nonparaneoplastic autoimmune retinopathy (np-AIR), the pediatric age of onset and hyperacute progression set HORD apart.
Further research is needed to determine HORD's etiology, optimal treatment strategies, and long-term prognosis. Identifying specific biomarkers, including potential novel antiretinal antibodies, may provide insight into disease mechanisms and therapeutic targets.
More information: Yizhe Cheng et al, Hyperacute Outer Retinal Dysfunction, JAMA Ophthalmology (2025). DOI: 10.1001/jamaophthalmol.2024.6372 Timothy M. Boyce et al, Hyperacute Outer Retinal Dysfunction—A Retina on Fire, JAMA Ophthalmology (2025). DOI: 10.1001/jamaophthalmol.2024.6488 Journal information: JAMA Ophthalmology
Timothy M. Boyce et al, Hyperacute Outer Retinal Dysfunction—A Retina on Fire, JAMA Ophthalmology (2025). DOI: 10.1001/jamaophthalmol.2024.6488
© 2025 Science X Network







Post comments